
Case
220 With discussion |
Versión
en Español |
|||
CASE 220 (June 2024)
Clinical information
A 14-year-old boy presents with nephritic syndrome. The mother reports a year of intermittent edema, with choluric urine, occasional headache, and no other symptoms. On physical examination, he was hypertensive, with facial and lower limb edema, and no skin lesions.
In paraclinical studies, normal hemoleukogram, serum cretinin: 1.8 mg/dL, BUN: 32 mg/dL, proteinuria 3.9 g/24h, sediment with 25 erythrocytes/CGA, without leukocyturia. Serum albumin: 2.4 g/dL. Dyslipidemia. ANAs and anti-DNA negative, C3: 22 mg/dL (88-180) C4: 16 mg/dL (15-40), virus studies negative, AELOS normal.
Kidney biopsy is done. Look at the images.
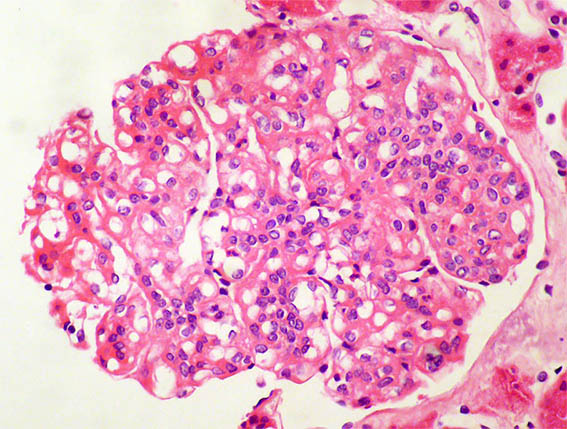
Figure 1. H&E, X400.
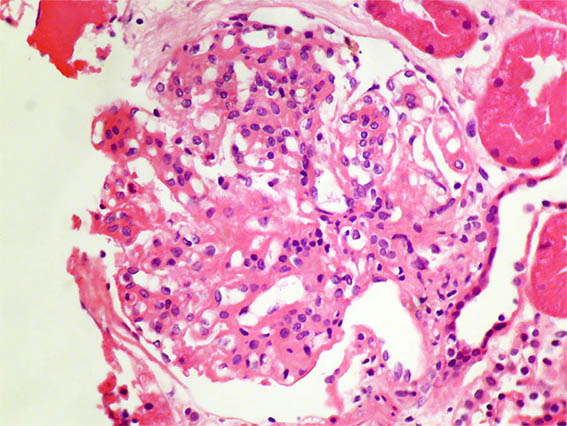
Figure 2. H&E, X400.
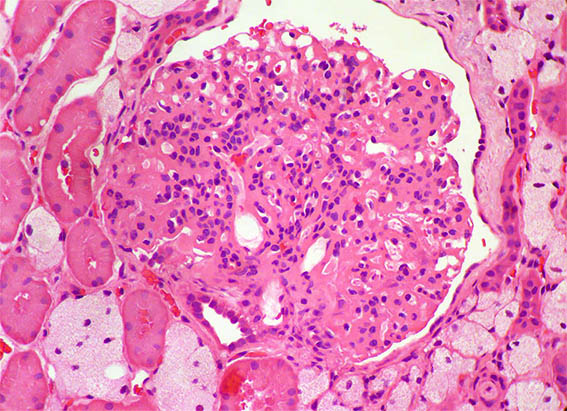
Figure 3. H&E, X400.
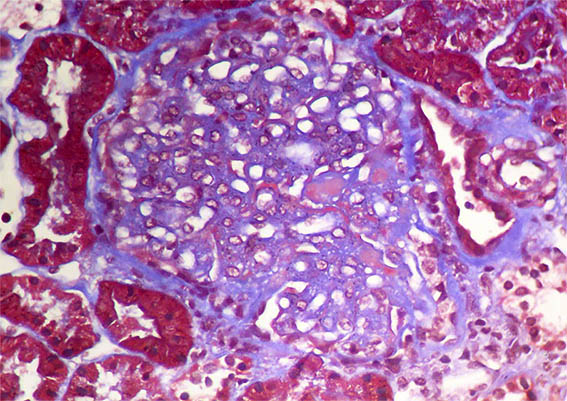
Figure 4. Masson's trichrome stain, X400.
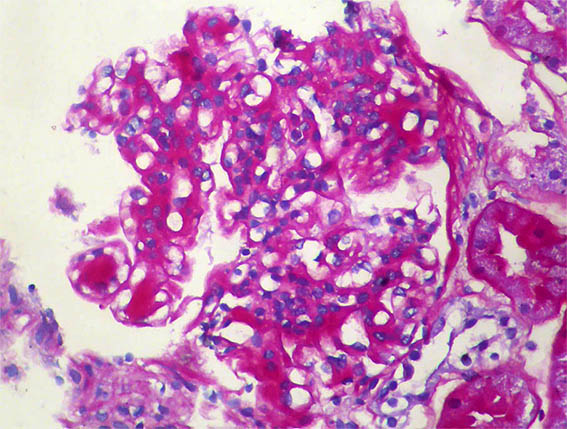
Figure 5. PAS, X400.
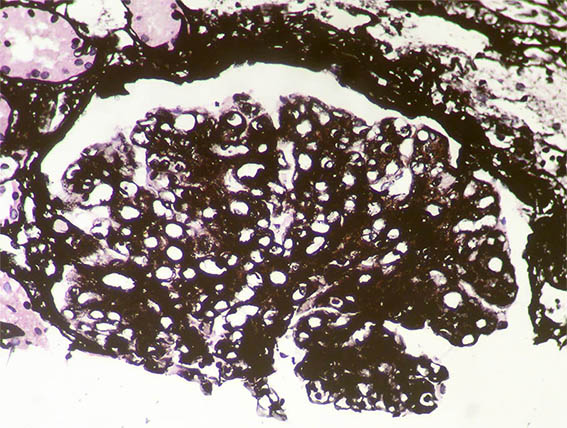
Figure 6. Methenamine-silver stain, X400.
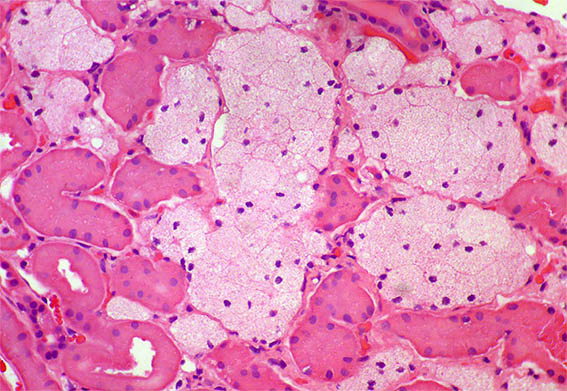
Figure 7. H&E, X400. Interstitium with foamy macrophages.

Figure 8. Direct immunofluorescence for IgG, X400. Negative
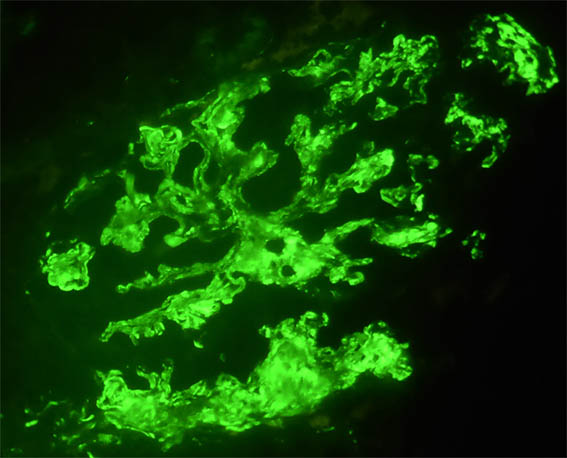
Figure 9. Direct immunofluorescence for C3, X400. Strong and diffuse subendothelial and mesangial positivity.
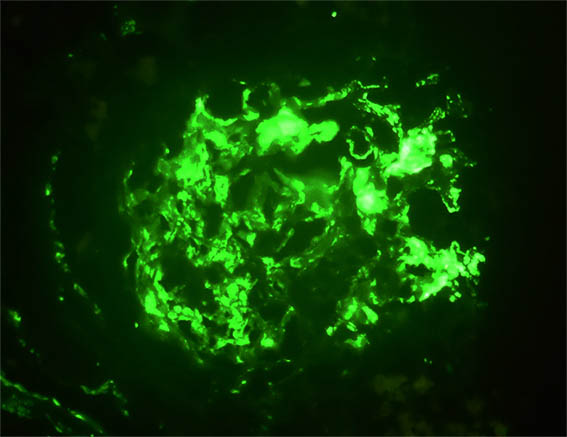
Figure 10. Another image of direct immunofluorescence for C3, X400.
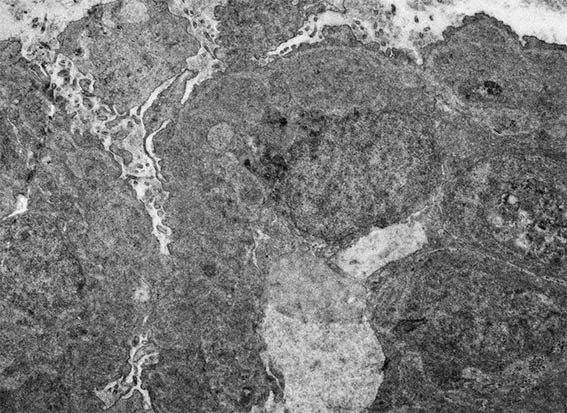
Figure 11. Electron microscopy, original magnification, X4,000. Note extensive podocyte damage, severe thickening of capillary walls, endothelial cell enlargement, and electron-dense subendothelial areas.
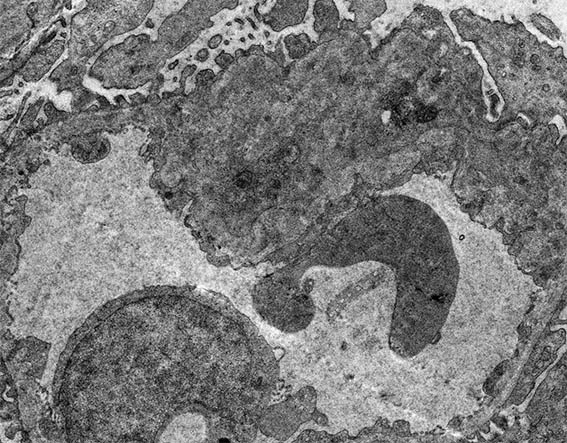
Figure 12. Electron microscopy, original magnification, X4,000. Segmental damage of the capillary wall, with a double contour.
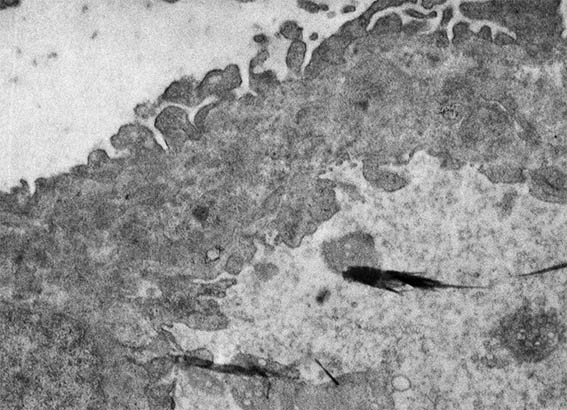
Figure 13. Electron microscopy, original magnification, X6,000. Basement membrane thickened with electron-dense subendothelial material alternating with small more electron-lucent areas.
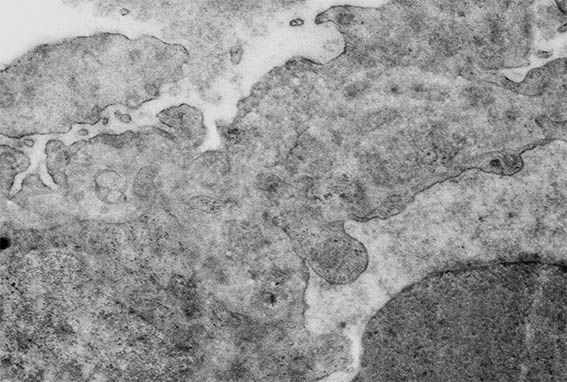
Figure 14. Electron microscopy, original magnification, X8,000. Basement membrane irregular, thickened, poorly defined.
Direct immunofluorescence for IgA, IgG, IgM, and C1q: Negative.
What is your diagnosis?